Pain Assessment Video (Start at 11:56 and end at 17:56): Pain Assessment in Visits/Assessments
Point of Care > Visits/Assessments > Pain screen. This screen has several tabs that run across the top of the screen. Some questions may differ depending on the payer type.

MainThe oasis questions will appear regardless of the assessment type that you have selected, but when shown as blue marks they are optional on visits that do not generate OASIS. If they were required, the indicators would be shown as red.
The Comments is a large text box that will allow you to document anything not covered. You can free hand type additional information here.
If the patient does not have any pain, you can indicate that here and also answer who provided the information. You can then move on to another area.
Pain Locations If the patient does have pain, you’ll need to indicate where and describe it. To do that, click the Pain Locations tab at the top. There are up to four spots to document pain location. If you have more than four locations, you can document more than one in the same location if they are close together. You can also add locations to the comments section.
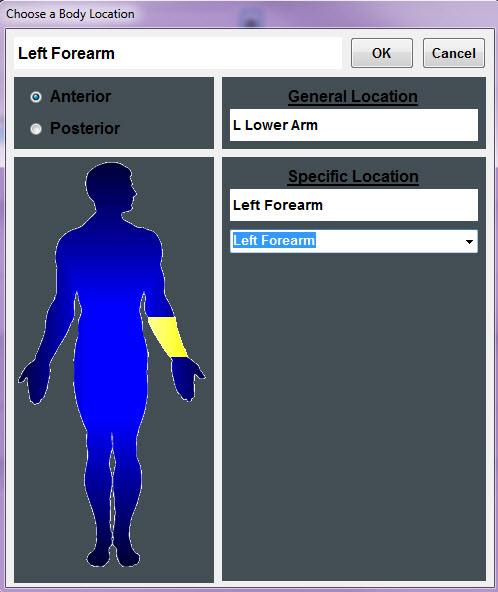
Click the asterisk button and you’ll see a diagram pop up for you to select a general location of the pain. Next, select Anterior or Posterior.
From the diagram, click the location of the pain. You’ll notice that the general location description shows up to the right. Use the drop down list to specify in more detail where the pain is located. Click the OK button when the information is complete. If you don’t find the location you need here, you can also type it in on the main pain location screen.
A common report from patients may be a headache. To document the pain location of a headache, click inside of the pain location field and type in headache.
Next, you will document the intensity by asking the patient to number the pain on a scale of 0 through 10. Document the description, exacerbated by, alleviated by and any additional comments you would like to document about the pain. The documentation for this pain location is finished.
Pain Meds Next, you can document how effective the patient’s medications are at controlling pain levels. Click the Pain Meds tab at the top of the screen. If the patient currently has pain medications listed in the Med History screen, they will show up at the bottom of the screen. If the patient is taking the pain medication to alleviate the pain you just documented, click on it and watch it appear at the top of the screen. The medication name and dose, freq, route will automatically appear. You can type in when the patient last took this medication. If the patient is taking a pain medication that is not listed on this screen, you can type the information in as well.
Answer the pain intensity questions for the level of pain before taking the medication, one hour after taking the medication and what pain level is acceptable. In the effectiveness box, you have the option to type in a description of your own description OR check the box for Meds are effective at controlling pain as observed and reported and watch it appear in the Effectiveness box. This description will appear on your visit note.
Nonverbal Assessment If the patient is non-verbal, you will use the Nonverbal pain assessment to indicate the level of pain. This section is used specific for pain assessment in advanced dementia patients and other non-verbal patients. There are five categories to observe. You can review the definition for each answer by clicking on the Definitions button within the category you are addressing. Once you review the information, click on the definitions button again to make it disappear.
Check the box for each observation. The top of the screen will calculate the pain score as you select your answers. The score of 0 equals no pain; the highest score of 10 would equal severe pain. This method is equivalent to that of asking the patient to pick a face or a number on a scale to describe their pain. The non-verbal pain score will print automatically on your visit note.
Teaching You can document pain-related teaching you provided for the patient by clicking on the Teaching tab. Check the box for any teaching given to the patient. Use the comment section at the bottom to document anything not covered in the top section.
History Use the History tab to see how the pain screen has been documented for this patient in the past. You can view the most recent seven assessments that have had pain documentation, or the first seven assessments with pain documented. You can also view all assessments that have pain documented.